
Nebula Genomics DNA report for RLS
Is RLS genetic? We created a DNA report based on a study that attempted to answer this question. Below you can see a SAMPLE DNA report. To get your personalized DNA report, purchase our Whole Genome Sequencing!

Additional Information
What is ALS? (Part 1 of Is ALS genetic?)
Amyotrophic lateral sclerosis (ALS) belongs to the group of motor neuron diseases and is a rare degenerative disease of the motor nervous system. It adversely affects nerves and the motor neurons. Hence, any activity that requires the use of voluntary muscles, like walking, talking or chewing, gradually weakens over time in this disease. This leads to progressive limitation in activities of daily living. Although there is no cure for ALS, how fast the disease progresses can be slowed down.
Other names for the disease are Lou Gehrig’s syndrome or Charcot’s disease. The latter was the describer of the condition, Jean-Martin Charcot. Lou Gehrig was a New York Yankees baseball player and had to retire after being diagnosed with ALS. Gehrig’s fate made the rare disease known to a large public for the first time. The famous Ice Bucket Challenge from 2014 was instrumental in raising funds towards ALS research (Information source: ALS Association: Ice Bucket Challenge).

.jpg){kind=link}
Research into the causes and potential treatments for the disease are ongoing. National organizations such as ALS Therapy Development Institute (TDI), the ALS Association, and the Centers for Disease Control and Prevention (CDC) all have funded projects in this area in 2020.
Epidemiology (Part 2 of Is ALS genetic?)
As of 2014, the CDC has reported 16,000 cases of ALS in the United States. An exact record regarding its very recent statistics is not much known. In the US, about 5-7 cases exist for every population of 1,00,000. It is in the age range of 55-75 years, that the disease is finally diagnosed. However, it’s worth noting that the condition rarely affects younger patients between 25 and 35 years of age. It is also more common in men than in women (the gender ratio is about 1.5:1).
Forms (Part 3 of Is ALS genetic?)
Primarily there are three main forms of ALS.
Sporadic ALS: This type occurs randomly without any probable cause. A majority (90 to 95%) of the ALS cases are sporadic. It is suspected that a combination of genetic and environmental factors are responsible.
Familial: In the U.S., the familial form of the disease is seen in a minority of the cases (5 to 10%), where people inherit ALS from a family member. Most cases are inherited in an autosomal dominant pattern, meaning one copy of the altered gene in each cell is sufficient to cause the disorder.
Guamanian: A Guamanian form of the disease has been observed in the population of Guam where the cause is the consumption of false sago palm, Cycas micronesia.
Pathophysiology of ALS (Part 4 of Is ALS genetic?)
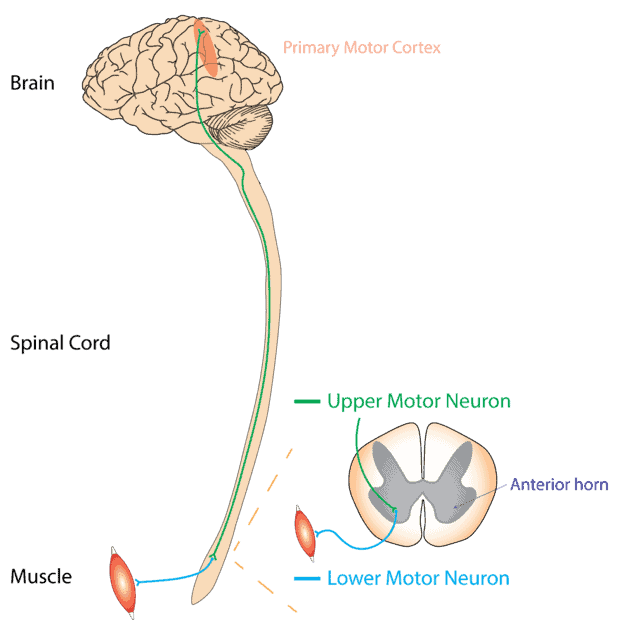
In ALS, both the upper and lower motor neurons in the brain and spinal cord are affected. The upper motor neurons occupy the brain while the lower motor neurons are in the spinal cord. According to the website of ALS Pathways, it usually spreads from a focal point thereby disrupting all the motor neurons in the body and ultimately causing the death of motor neurons. And multiple factors are responsible for this type of neurodegenerative disease. Other forms may only affect the upper motor neurons (primary lateral sclerosis, PLS) or the lower motor neurons (progressive muscular atrophy, PMA).
The degeneration of the upper motor neurons leads to increased muscle tone or spastic paralysis. While the damage of the lower motor neuron leads to an increase in muscle weakness. This interferes with the proper functioning of daily activity.
{kind=link}
Causes (Part 5 of Is ALS genetic?)
In ALS, genes are suspected to play a role in the risk of developing the disease. Studies strongly support genetic factors linked to ALS. However, studies implying the role of some of the environmental factors are not very consistent. In a majority of cases, the exact cause is not known. But in the rest of the small cohort (5-10%), genetic factors may explain the condition. Other factors such as family history, gender, geography, etc. might also have associations with ALS.
Is ALS genetic?
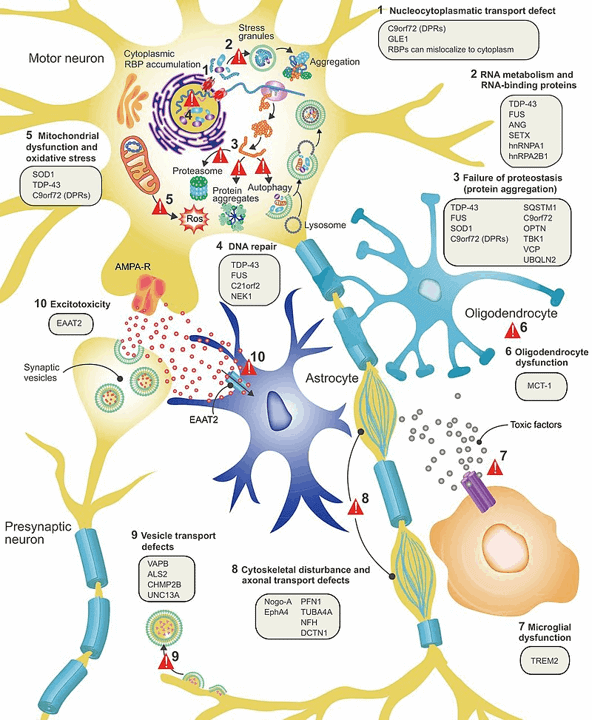
A number of genetic variants are closely linked to ALS. Specific gene mutations associated with the disease lead to the pathological accumulation or premature degradation of misfolded proteins which ultimately triggers neurodegeneration.
Major genetic components in ALS
SOD1
The SOD1 gene codes for an enzyme known as superoxide dismutase. This enzyme plays an important role in the anti-defense mechanism. The misfolded variants of SOD1 proteins lead to progression.
TARDBP
This gene encodes TDP-43, a protein that regulates gene expression. TDP-43 is crucial to various stages of RNA processing. Some dominant genetic mutations in TARDBP results in faulty TDP-43, thereby causing neurodegeneration. Hence, changes in the distribution and functions of this protein have a strong association with ALS.
FUS
The FUS gene expresses the FUS protein which is a type of RNA binding protein. Some of its functions are similar to those of the TDP-43 protein. Therefore, the FUS protein monitors a number of processes in RNA metabolism. In ALS, pathogenic variants of this gene sometimes cause improper folding and distribution of the FUS protein, thereby interfering with the normal cellular physiology.
C9ORF72
Although the exact role of this gene is not yet clear, few reports have indicated its involvement in protein transport especially in the form of endosomal activity and autophagy. And a decreased expression of C9ORF72 might be associated with disease, as noted in a few animal studies. However, this downregulation alone does not result in ALS, but in fact, works in a complex of a few other proteins.
Minor genetic components of ALS
Few other genetic modifiers in ALS are ATXN1, ATXN2, UNC13A. Mutations in these genes likely make people susceptible to the disorder. But they do not strongly correlate with this disease.
Non–genetic component of ALS (Part 7 of Is ALS genetic?)
Occupational risk factor
A number of reports have proposed that professional athletes are most likely to develop ALS. And this could be mainly due to severe head injuries or intense physical activities.
Other examples of workplace exposure are cases where people are exposed to magnetic fields or strenuous physical work. However, such studies are association based, not consistent, and with unknown etiology.
Toxic chemicals
The results of a study at the University of Michigan in Ann Arbor (May 2016) confirmed the long-standing suspicion that exposure to environmental toxins may increase the risk of developing ALS. In this study, the researchers observed a significant association between the disorder and the presence of chlorinated hydrocarbons, polychlorinated biphenyls and polybrominated biphenyls.
Beta methylamino L-alanine (BMAA)
BMAA is a neurotoxin associated with ALS. An indigenous population living in Guam has been reportedly at a heightened risk of having the disease. The diet of this population is rich in BMAA. Generally, cyanobacteria in the Pacific islands water produce BMAA. And given that the people of Guam depend on seafood, this may put the population at a higher risk.
Microbiome
The gut microbiome often influences the disease outcome, as reported in animal studies. Gut microbiome studies in mice have demonstrated that there is an important link between some of the bacterial strains and ALS. Moreover, in this study, a strain of Akkermansia muciniphila tends to slow down the progress of the disease in mice. Another 2020 study in mice has reported that gut microbial communities influence the survival outcome. This was especially noted, because the ALS-susceptible mice, despite having similar genetic backgrounds, showed significant differences in lifespan. The diversity patterns of the microbial communities were significantly different – one of the factors that could have contributed towards the differences in the survival span of those mice.
Symptoms (Part 8 of Is ALS genetic?)
The hallmark symptoms of ALS are functional impairment of the muscle movement in the upper and lower extremities, the bulbar muscles, and the trunk muscles.
According to the National Institute of Neurological Disorders and Stroke, symptoms accumulate gradually. Some early symptoms of ALS include:
- Fasciculations (muscle twitches) in the arm, leg, shoulder, or tongue
- Muscle cramps
- Tight and stiff muscles (spasticity)
- Muscle weakness affecting an arm, a leg, neck or diaphragm
- Slurred and nasal speech
- Difficulty chewing or swallowing
Depending on the first symptoms observed, the condition can be further divided into subcategories. When symptoms first begin in the arms or legs, it is known as “limb onset” ALS. If the first indications are speech or swallowing problems, it is referred to as “bulbar onset” ALS.
ALS progresses differently in different individuals. However, in all cases, muscle weakness and atrophy spread to other parts of the body until functioning becomes difficult. People with advanced stages of the disease will eventually not be able to stand, walk or use their limbs and swallowing, speaking, and breathing may become difficult.
In most cases, people with ALS retain their ability to perform higher mental processes such as reasoning, remembering, understanding, and problem solving.
The average survival time of the patient is about three to five years from the onset of the disease, however, 10-20 percent of patients can survive for a longer duration.
Diagnosis (Part 9 of Is ALS genetic?)
Mostly, the symptoms vary from one person to another. Hence, a doctor will conduct a thorough examination using multiple tests. As of now, there is no clinical genetic testing for ALS.
Physical examination: In most cases, increasing muscle weakness, muscle atrophy, or even muscle twitches lead patients to a doctor for the first time. It should be noted that muscle twitches alone almost always represent benign fasciculations. At first, the symptoms can appear anywhere on the body. During the examination, the simultaneous appearance of signs of flaccid and spastic paralysis reinforces the suspicion of the diagnosis of ALS.
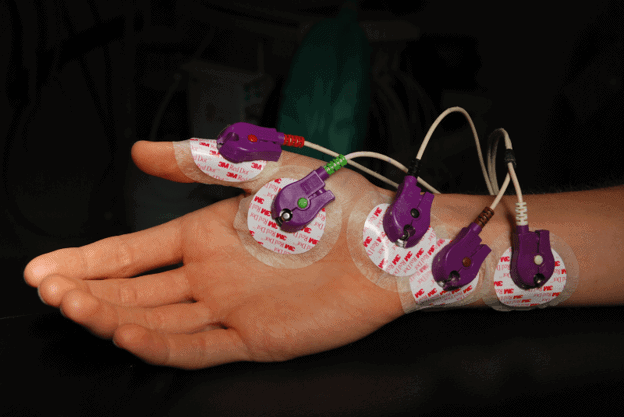
Electromyography: An electromyographic and electroneurographic examination is indispensable for making a diagnosis. Electromyography analyses the electrical activity in the muscles. Internationally standardized criteria have been developed for making the diagnosis (El Escorial criteria). According to these criteria, a diagnosis requires examining the degeneration in the upper and lower motor neurons, their progress, and also the absence of any other neurodegenerative disease.
{kind=link}
Spinal tap: The physician draws out a small volume of cerebrospinal fluid and looks for the presence of inflammatory conditions or abnormal cells. This test is important only in cases with unusual symptoms.
Biopsy: Generally, a surgeon removes a part of the muscle from the upper arm or upper thigh. The surgeon then looks for any damage using staining and microscopy.
Treatment (Part 10 of Is ALS genetic?)
Usually, treatment comprises a combination of drug therapy and symptomatic oriented therapy. Symptomatic therapy intends to help avoid complications of muscular weakness and improve the patient’s quality of life. In animal models and human stem cells, genetic studies have identified potential drug targets, which could be a step forward towards developing drug therapy.
Sometimes, people might want to undergo genetic testing especially in cases with a family history of ALS. Then, in such cases, the genetic counselor may help in evaluating not only the family history, but also the medical background, and any other potential risks. For familial ALS, a positive test result is usually observed in 60-70 percent of the cases.
Neuroprotective therapy
Riluzole is the common drug in neuroprotective therapy. This drug inhibits the destruction of motor nerve cells by blocking the release of the neurotransmitter glutamate from neurons.
The administration of riluzole reportedly prolongs survival by about three months and prolongs the earlier stages of ALS. However, it should be noted that the progression of the disease cannot be entirely stopped by riluzole.
As of 2017, the US Food and Drug Administration has granted the approval of yet another drug Edaravone. It indicatively slows down ALS development.
Symptom therapy
The following symptoms are often treated with appropriate therapies:
- Muscle cramps
- Dysphagia
- Salivation
- Speech disorder and communication
- Pathological laughter and crying
- Respiratory disorders
- Depression, sleep disorder, and anxiety
Recent news (2020)
Researchers at Trinity College Dublin have initiated the Phase 1 clinical trial of gene therapy at the Clinical Research Facility, St. James Hospital Dublin (as of September 1, 2020). This gene-based therapy targets the gene C9ORF72. The U.S. pharmaceutical company Biogen has sponsored this clinical trial.
Did you like this article? Be sure to check out the other posts in the Nebula Research Library!