
Table of contents
- Insomnia Genetic Report
- Insomnia Information
- Definition of Insomnia
- Classification systems of Sleeplessness
- Clinical manifestations of insomnia
- Consequences of sleep deprivation
- Distribution of Insomnia
- Sleep disorders in children
- Structural anatomical changes
- Cause
- Sleep disorders in depression and anxiety disorders
- Origin of the disease
- Types of insomnia
- Therapy
- Prevention
- Misconceptions about sleep
- Treatment of Insomnia
- Urban Myths
Insomnia Genetic Report
SUMMARY: This study identified several genetic components that were associated with insomnia genes, including 2 that were gender-specific.
DESCRIPTION: Insomnia is a sleep disorder that makes it difficult to fall or stay asleep. In a genome-wide association study, researchers examined genetic variants associated with chronic sleep disturbances, which affect 25-30% of adults worldwide. The study examined 503,325 people living in the United Kingdom in order to analyze data of several genetic variants linked to insomnia, which explained roughly 21% of the heritability for insomnia symptoms based on nature genetics. Lane and Massachusetts General Hospital identified 57 loci related to insomnia to answer the question is insomnia genetic. Interestingly, this study also found one variant (in the TGFBI gene) significantly associated with insomnia only in females and another (in the WDR27 gene) that was only significant in males. The TGFBI gene plays a key role in cell adhesion, while the exact function of the WDR27 gene is relatively unknown. However, it is thought to be involved in cell signaling and protein-protein interactions.
DID YOU KNOW? To try and prevent insomnia, you should avoid caffeine, alcohol, and heavy meals late in the day. Try to go to bed and get up at the same time each day. If you have trouble falling asleep, try relaxing before bed by reading a book, taking a bath, or making a to-do list if you’re worried about the things you need to do in the morning. [SOURCE]
SAMPLE RESULTS: Learn more about the Nebula Research Library.

INSOMNIA-ASSOCIATED VARIANTS: rs113851554, rs5922858, rs145258459
ADDITIONAL RESOURCES:
An Overview of Insomnia
Cell Adhesion
Introduction to Cell Signaling
WEEKLY UPDATE: July 23, 2019
Insomnia Information
This article describes insufficient sleep in humans. The term sleep disorder (syn. agrypnia, insomnia and hyposomnia) describes differently caused impairments of sleep. The causes can be external factors (such as night-time noise, street lighting that is too bright), behavioral factors (e.g. problematic sleep hygiene) or biological factors.
The lack of restorative sleep impairs performance in short term insomnia and can also lead to the worsening or reappearance of diseases in the long term. Sleep disturbances cause illness if they cause physical or mental impairments and are also perceived by those affected as pathological. The opposite sleep behavior, sleep addiction (technical term hypersomnia), can also be a consequence.
Pathologically increased daytime drowsiness (e.g. assessable using the Epworth drowsiness scale) is in most cases caused by a treatable biological disturbance of sleep quality. These include sleep-related breathing and movement disorders.
In order to differentiate between the individual subtypes of sleep disorders, it is particularly important to carefully take a medical history and, of course, to carry out further examinations, for example in a sleep laboratory. The treatment is essentially oriented towards the causes. For example, if the sleep disorder is the result of an internal disease, its treatment is given priority. However, if it is caused by an incorrect approach to sleep, a corresponding explanation to the patient and – if necessary – behavioral therapy is suggested.
Definition of Insomnia
Insomnia describes not only the absence of sleep, but also disorders of falling asleep and sleeping through, as a result of which the affected persons have not slept in the morning. Hyposomnia also stands for “too little” sleep in the sense of insomnia or “light insomnia”. In addition, the term insomnia is also used when sleep is completely absent, for example in the case of fatal familial insomnia.
Dyssomnia is the generic term for a disturbed sleep behavior. This includes both “too little” and “too much” sleep in terms of depth and duration. The term thus covers sleep disturbance and sleep addiction.
Hypersomnia refers to sleep or bed addiction, in which the person affected has a significantly longer need for sleep than normal people. The need to sleep can also occur during the day or in attacks (catalepsy).
Idiopathic insomnia is also known as insomnia in childhood and lifelong insomnia. A cause for this form of the disease is not known.
The pseudo-, subjective or paradoxical insomnia describes a subjectively experienced sleep disorder without objective findings. As a further term for it, misperception of the sleep state or the term “sleep state misperception” can be found in the literature.
Insomnia caused by mental illness is also called psychiatric insomnia or, in the case of depression, depressive insomnia.
Classification systems of Sleeplessness
Classification according to ICD-10
F51 non-organic sleep disorders
F51.0 non-organic insomnia
F51.2 Non-organic disturbance of the sleep-wake rhythm
F51.3 Sleepwalking (somnambulism)
F51.4 Pavor nocturnus
F51.5 Nightmares (anxiety dreams)
G47 Sleep disorders
G47.0 Sleep-in and sleep-through disorders
G47.2 Disturbances of the sleep-wake rhythm
G47.3 Sleep apnea
ICD-10 online (WHO version 2019)
There are different classifications with the aim of schematically depicting sleep disorders. This process is in a state of flux, the classifications were sometimes quite short-lived or are used next to each other. Likewise, the use of terms used in connection with sleep disorders is not uniform. The corresponding AWMF guideline is also currently being revised.
The following classification systems are available for the classification of sleep disorders:
ICD-10 (International Classification of Disorders, WHO, 1993)
DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, American Psychiatric Association)
ICSD (International Classification of Sleep Disorders, 1990), ISCD-R (1997), ICSD-2 (2005)
ICD-10
According to ICD-10, sleep disorders are classified according to their presumed cause (psychogenic versus organic) as F51 non-organic sleep disorders (chapter on psychological and behavioral disorders) or G47 (organic) sleep disorders (chapter diseases of the nervous system).
Non-organic dyssomnias are primarily psychogenic disturbances of the duration, quality or timing of sleep due to emotional causes that are present to a considerable extent (at least three nights a week for a period of at least one month), cause significant suffering and/or have a disturbing effect on everyday functioning (daytime tiredness).
Non-organic insomnia (F51.0): the main features are difficulties in falling and staying asleep and poor sleep quality (non-restorative sleep).
Non-organic disturbances of the sleep-wake rhythm (F51.2): the sleep patterns deviate from the desired sleep-wake rhythm (which is determined by social requirements and shared by most people in the affected person’s environment), consequently insomnia during the main sleep period and hypersomnia during the waking period.
Non-organic parasomnias are abnormal episodes that occur during sleep. Sleepwalking (F51.3): repeated episodes (two or more) in which the affected person leaves the bed during sleep and walks around for several minutes to an hour, usually during the first third of the night’s sleep. During this episode, the affected persons usually have an empty, rigid facial expression, hardly react to other persons and can only be awakened with great effort. After waking up, the affected persons do not remember the episode (amnesia), otherwise there is no impairment of mental activity or behavior after waking up (except for a short phase of confusion or disorientation).
Night terrors (Pavor nocturnus) (F51.4): repeated episodes (two or more) in which the affected person (usually in the first third of sleep) wakes up from sleep with a panicky cry, accompanied by severe anxiety, body movements and vegetative overexcitement (tachycardia, rapid breathing, sweating). Efforts by others to influence the person during the episode are unsuccessful or result in disorientation and perverse movements. An episode lasts up to 10 minutes.
Nightmares (F51.5.): Waking up from night sleep or afternoon sleep with detailed and vivid memories of severe anxiety dreams. These are usually about threats to one’s life, security or self-esteem and cause considerable suffering for those affected. After waking up from the anxiety dream, the affected persons are quickly oriented and awake.
Organically induced sleep disorders include difficulties falling and staying asleep (G47.0), disorders of the sleep-wake rhythm (G47.2) and sleep apnea (G47.3).
Primary sleep disorders are divided into dyssomnias and parasomnias. Dyssomnias include primary insomnia, respiratory-related sleep disorders (unless caused by another disease or substance intake) and sleep disorders due to a disturbance of the circadian rhythm. Parasomnias include sleep disturbance with nightmares, Pavor nocturnus and sleep disturbance with sleepwalking (somnambulism).
Furthermore, it is subdivided into sleep disorders that occur in connection with another mental disorder: those that occur due to a medical condition and those that are related to the use of a psychotropic substance such as alcohol, amphetamine, caffeine, cocaine, opiate or medication (substance-induced sleep disorder).
DSM-5
While older diagnostic systems attempt to distinguish between primary and secondary insomnia based on the cause, the DMS-5 is limited to a purely descriptive approach. It is assumed that medical problems and psychiatric disorders can be a cause and consequence of sleep disorders, which results in unreliable criteria in individual cases [16].
The DSM-5 defines insomnia as an unsatisfactory amount or quality of sleep: difficulty falling asleep and/or
difficulty sleeping through the night and/or premature awakening without being able to fall asleep again. Sleep disorder is considered a disease if it leads to significant discomfort or impairment of the ability to cope with the day, e.g. by (at least one criterion):
Exhaustion, lack of energy
Drowsiness during the day
decreasing attention, concentration, retentiveness
vocational or school performance reduction
deteriorated communication or social behavior
deteriorated care or family activity.
ICSD-2
According to the International Classification of Sleep Disorders (ICSD-2) of 2005, sleep disorders can be divided into 8 groups including insomnia (with different causes), sleep-related breathing disorders (e.g. sleep apnea), circadian sleep-wake rhythm disorders (as in shift work or jet lag), parasomnias (e.g. (e.g. sleepwalking, Pavor nocturnus, nightmares), sleep-related movement disorders (e.g. restless legs syndrome, bruxism), isolated symptoms, apparently normal variants and unexplained problems (e.g. snoring, talking during sleep) and other sleep disorders (e.g. environmental sleep disorder, noise). As the eighth group, ICSD-2 also lists sleep addiction (hypersomnia) of central origin, not caused by circadian rhythm disturbances, sleep-related breathing disorders or other causes of sleep behavior disorder.
Clinical manifestations of insomnia
The symptoms of non-restorative sleep correspond in essential aspects to those of sleep deprivation.
The main symptom of a sleep disorder is the lack of restful sleep. This term includes delayed falling asleep, disrupted sleep through and waking up too early. If sleep is unpleasant, more or less intense drowsiness can also occur during the day, reducing alertness and the ability to maintain vigilance. In addition, those affected can also have a strong urge to fall asleep during the day. Other typical symptoms include irritability, restlessness, anxiety and other symptoms generally associated with fatigue, ranging from a decline in performance to a change in character. In severe cases, these symptoms in particular also impair the patient’s social and professional situation.
The symptoms must occur on three days of a week for at least one month in order to be considered as pathological. If the sleep is not restful during this time, the performance and well-being are impaired during the day, and they are described as severe. Specifically, a healthy person should fall asleep at least 30 minutes after going to bed, not be awake earlier than 30 minutes after falling asleep (up to 2 hours for older people) and not wake up before 5:00 a.m. (without being able to fall asleep again).
Very similar clinically, idiopathic, learned and sometimes pseudo-insomnia are very similar, which is why they are often difficult to distinguish.
An unsolved problem is the discrepancy between the subjective perception of sleep quality and the objective results of polysomnography (PSG). In contrast to healthy sleepers, people with sleep disorders experience the waking phases longer than measurement of PSG showed. This led to the term paradoxical imsomnia. More detailed analyses revealed that people with insomnia perceived waking up from REM sleep (usually associated with dreaming) as a long waking period, but not waking up from an N2 sleep phase.
In pseudo-insomnia, clinical findings such as reduced performance do not correlate with the sleep disturbance experienced by the patient. However, those affected suffer from increased anxiety, especially about their own health, and depression. They also have an increased risk of misuse of drugs or other substances.
Schenck syndrome, which occurs almost exclusively in men, carries a considerable risk potential. If, for example, the bed partner is mistaken for an attacker, he or she can be injured in the process. Statistically speaking, in about two-thirds of the cases, partners are at risk, in about one-third of the cases, self-endangerment occurs; in 7%, even bone fractures occur.
Consequences of sleep deprivation
There are many studies on the psychological and physical effects of sleep deprivation. In a major study by the American Cancer Society, over one million participants were asked only about their average length of sleep. It showed that participants who slept less than 6 hours and more than 9 hours per night showed a higher mortality rate than expected for their age. Other studies were able to document the psychological and physical consequences of sleep deprivation more accurately: Sleepiness, lack of concentration and attention, irritation, anxiety, depression, mood swings, lack of self-esteem, impulsiveness and impairment of social relationships. Well-studied physical consequences of sleep deprivation include obesity, impaired glucose tolerance and higher levels of diabetes, hypertension, heart attack and stroke.
Distribution of Insomnia
Most people’s expectations of good night’s sleep are simple: they want to fall asleep quickly, sleep well through the night and wake up in the morning “full of energy”. More or less pronounced sleep disorders are a common phenomenon that is subjectively perceived and judged by the patient. Even those who do not wake up well-rested every morning can in some cases experience this as a sleep disorder. The frequency of occurrence in the population ultimately depends on how one defines sleep disorder. It ranges from just under 4% to about 35%.
The question of when disturbed sleep can be considered a pathological sleep disorder from a medical point of view cannot therefore be answered in a generally valid way. In practice, however, it can be assumed that about 20 to 30% of all people in western industrialized countries, like the United States, have more or less pronounced sleep disorders. About 15 % of them also suffer from tiredness during the day and a general limitation of their performance, so that treatment is indicated here. Noteworthy sleep disturbances caused by bad sleeping habits alone account for about 2 % of all adolescents and young adults. Objective disturbances of the sleep-wake rhythm are rare. A too late time for falling asleep, the so-called delayed sleep phase syndrome, is found in about 0.1% of the population, a too early (pre-shifted sleep phase syndrome) in about 1%.
Typically, older people wake up several times during the night and have a lighter sleep overall (lower wake-up threshold). However, these changes alone are not perceived as pathological by the vast majority of those affected. At the same time, existing health problems as well as the influences of the environment and social situation are considered to be essential influencing factors. Abnormalities during sleep (parasomnias) occur more frequently in childhood. A characteristically only after the 60th year of life (scarcely 90%) occurring parasomnia is with men (scarcely 90%) the relatively rare (0.5% of the population) Schenk syndrome.
100 % of all people experience a nightmare at some point in time, about 5 % of all adults develop a considerable amount of suffering due to nightmares. About 1 to 4 % suffer from sleepwalking, sleep disorders caused by eating or drinking at night or night terrors. About every third sleep disorder, an estimated 30% of the total population, is caused by a psychiatric form of the disease, for example depression.
Acute sleep disorder, which is triggered by stress in the short term, affects an estimated 20% of all people every year and can occur in all age groups, but is more common among older people and women. The psychophysiological (learned) sleep disorder affects about 1-2 % of the population. Quite rare (about 5 % of all sleep disorders) is also pseudo-insomnia, where the affected persons only have the feeling of sleeping badly, but this cannot be objectified.
Idiopathic or even lifelong insomnia without known cause affects less than 1% of all children and young adults. Congenital fatal familial insomnia occurs in less than one in one million people.
Sleep disorders in children
Overview
Basically, children can have essentially the same types of sleep disorders as adults. However, parasomnias make up a larger proportion in this age group. These subclass of insomnia include premature infant apnea, attributed to the immaturity of the respiratory center in the brain stem. Although it primarily affects underweight premature babies (occurring in about 85% of all babies under 1000 g), it also plays a role in everyday life. For example, it is estimated that about 2% of all children born on time and in good health will experience at least once in the first six months of life an episode of at least 30 seconds of respiratory arrest and at least 20 seconds of a drop in heart rate to below 60 beats per minute. Other parasomnias typical of childhood include obstructive sleep apnea syndrome and primary alveolar hypoventilation syndrome.
Insomnia in Childhood
Insomnia in childhood (protodyssomnia) is also a behavioral insomnia. Falling and staying asleep are the main symptoms. There are two main groups to be distinguished. For example, the sleep onset association type (translated as “organized falling asleep type”) requires certain objects and rituals in order to find sleep. In the limit-setting type, an excessively generous upbringing leads to a refusal to accept the child, which in the end also culminates in sleep disorders.
Today, two doctrines dominate the literature on behavioral insomnia: Some research-oriented authors, including Richard Ferber, for example, attribute the insomnia of many children to their educational inability to calm themselves, and recommend that the parents of such children train their ability to find their way to sleep on their own. Gentle, but consistent, training can help the child to become independent of the often excessive parental micromanagement of childhood fatigue. Others, however, especially attachment parenting supporters such as William Sears, consider insomnia to be anxiety-related and recommend co-sleeping.
The clinical symptoms of sleep disorders in children are very similar to those of adults. In addition, however, not only the child but also the parents suffer considerably. This can result in negative, aggressively occupied emotions towards the child, or even threatens the parental partnership.
Structural anatomical changes
In chronic insomnia, structural anatomical changes in the brain have been detected by MRI. Specifically, this involves a reduction in the size of the hippocampus. Although this is probably not true for all forms of primary sleep disorder, this fact has been reproduced in two independent studies, at least for patients with increased nocturnal activity.
In hereditary fatal familial insomnia, a sponge-like change in the brain is found. Particularly conspicuous are gliosis and the loss of nerve cells, especially in the area of the anterior and dorsomedial thalamus nuclei. This disorder is
Cause
Sleep disorders for which no cause can be found are also called primary or idiopathic. Secondary are those with reasons that are comprehensible. A special form is parasomnia.
In addition, extrinsic and intrinsic disorders can also be distinguished. The former include all causes that originate outside the patient’s body, such as alcohol, lack of sleep or environmental influences such as light pollution. Possibly the radiation of cell phones is also among them. Also impairments of the circadian sleep rhythm such as jet lag (change of time zone) and the sleep phase syndrome (advanced or delayed) are usually included. For example, primary insomnia, sleep apnoea syndrome and restless legs syndrome are described as intrinsic.
Another special feature is pseudo-insomnia. With this misperception of the sleep state, night sleep in the sleep laboratory is completely regular and normal, but when waking up, the affected persons have the feeling that they have not slept at all or only badly.
Sleep disorders in depression and anxiety disorders
There is a scientifically established link between sleep disorders – especially insomnia – and depression. Insomnia is often found in patients with a diagnosed clinical depression, where it is considered the core symptom. Anxiety disorders can also be accompanied by insomnia. Vice versa, people with insomnia more often develop depressive disorders and anxiety disorders.
People with depression respond more slowly to the treatment of insomnia than other patients with insomnia.
Origin of the disease
In order to be refreshing, sleep must be sufficiently long and have as undisturbed a course as possible. In particular, the deep sleep phases must also be available in sufficient quantity. In depressive patients, for example, they are significantly reduced. Those affected wake up more often at night than healthy persons, REM sleep not only occurs more frequently and prematurely, but is also accompanied by particularly intensive eye movements. 90% of all depressive patients do not have restful sleep. The fatal familial insomnia is also characterized by an increasing loss of K-complexes and delta waves. REM sleep may also be altered in this disease.
In learned insomnia, a disturbed sleep process (delayed falling asleep, more light sleep and less deep sleep), increased secretion of cortisol and interleukin-6, changes in anatomical structures in the brain, and a normal or increased tendency to fall asleep during the day have been found.
Idiopathic insomnia is widespread – in some cases already in childhood – with a longer period of time until falling asleep, increased lying awake at night and consequently with a shortening of the total sleeping time. In addition, deep sleep phases (stages III and IV) are significantly reduced compared to light sleep (stages I and II).
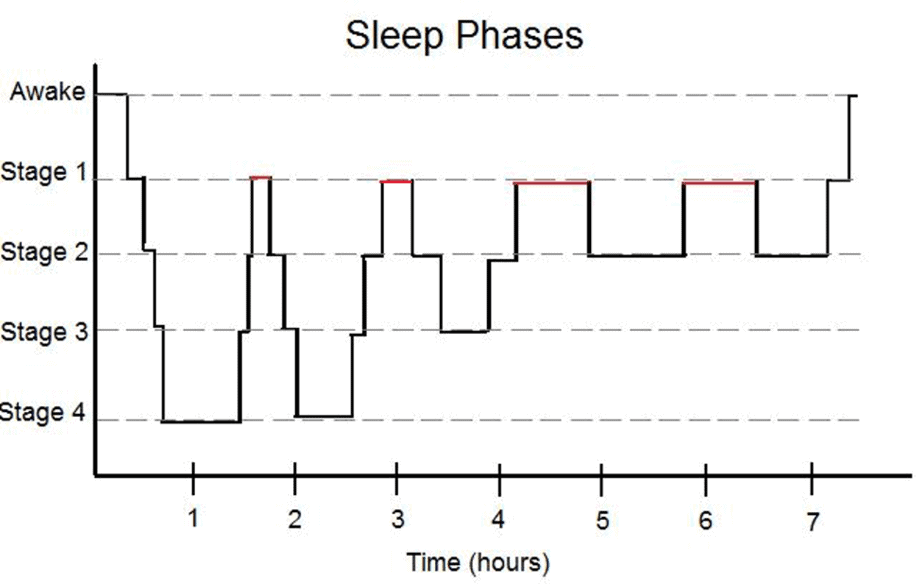
The stages of sleep as depicted in a healthy sleep cycle. Image credit Kernsters.
In restless legs syndrome, continuous nocturnal movements result in deep sleep stages III and IV not being reached, or being reached only very rarely, compared to healthy sleep, and those affected wake up significantly more often.
In the case of time shifts, such as those that occur during shift work or air travel, the light-dark rhythm of the times of day, the circadian rhythm of numerous bodily functions and the “clock genes” innate to humans as day-active beings influence the course of sleep. Here too, deep sleep decreases in duration and intensity. Predisposition, long-term disturbances of the light-dark rhythm, inadequate sleep hygiene and the compensation of insufficient sleep quantities on previous days are discussed for the similar but chronically proceeding changes in the times of falling asleep.
In contrast to the other forms of sleep disorders, there are no objectifiable findings in the sleep laboratory for pseudo-insomnia. Nevertheless, those affected perceive their sleep as not restful.
Types of insomnia
Primary insomnia is defined by the fact that no concrete causes are found.
Causes for secondary, i.e. acquired insomnia are, for example, diseases or substances that have a correspondingly negative influence on the sleep phases. This is quite easy to understand in the case of diseases such as benign enlargement of the prostate gland or heart failure, which can lead to frequent urination at night. As a result, the night’s sleep is interrupted several times and loses its restfulness.
It is similarly easy to understand when there are short-term changes in the internal clock and thus in the sleep-wake rhythm, whereby – colloquially expressed – night sleep becomes midday sleep and thus has a different sequence (for example, fewer deep sleep phases). Analogous changes can also be seen in shift work, when the actual sleeping time becomes working time. It is rarer, but similar in people who have a normal sleep but whose internal clock is slowing down or advancing for unexplained reasons (chronic sleep-wake-rhythm disorder), who for example can only fall asleep between one and six o’clock in the morning and would then have to sleep until noon in order to achieve a sufficient amount of sleep for recovery. Each of the three forms of chronic sleep-wake-rhythm disturbances can be caused in the same way by diseases such as fibromyalgia, dementia, personality and obsessive-compulsive disorders or by taking medication such as Haloperidol and Fluvoxamine or drugs.
Depression is associated with sleep disorders in the vast majority of patients. A relative predominance of the cholinergic system and a deficient function of REM sleep are considered to be the cause.
Stress can severely impair night sleep. The stress can be caused by disturbances in the social environment or in the occupation (this includes long-term factors, but also short-term ones such as standby or emergency doctor service times), but also by moving house, changes in the environment when sleeping or the occurrence of serious physical illnesses as well as in a broader sense also after previous excessive physical strain. Due to stress, these patients often brood during the day and are affected by anxiety, sadness and dejection. The symptoms usually end when the circumstances are of little or no importance to the person in question, which is why this form is also known as adaptive, transient, transient or acute insomnia. This stress-related form is considered a common cause of insomnia, which is referred to as learned, chronic, conditioned, primary or psychopathological insomnia, in which the person affected internalizes associations that affect sleep or lead to awakening, i.e. learns that restful sleep is no longer possible. In the long term, this developing insomnia also leads to irritability, impairment of mood, performance, concentration, motivation and attention. Typically, these patients do not even take a nap during the day.
Further causes are in particular internal, neurological and psychiatric clinical pictures such as varicose vein diseases, hyperthyroidism, reflux disease, chronic pain syndromes, psychoses, epilepsy, dementia and Parkinson’s disease, which can impair sleep.
Therapy
Research methods
When patients seek medical advice and report unpleasant sleep, problems with falling asleep or sleeping through the night, early awakening or drowsiness during the day, by which they feel considerably impaired, then a variety of very different reasons can be considered in addition to a sleep-related illness.
These can include false expectations of sleep as well as behaviors and living conditions that no longer allow sleep to be restful. In such cases, education about correct behavior according to the rules of sleep hygiene can be helpful. It must also be clarified whether the taking of medication or other substances that impair sleep is the cause. In such cases, it may be advisable to switch to other medication. If substances are known to cause addiction, weaning may be necessary. If there are indications of a secondary sleep disorder whose trigger is another existing illness, the causative illness must be treated accordingly.
If up to this point no causes for the complaints can be identified, a primary sleep disorder requiring treatment may be suspected and a corresponding specific procedure in terms of diagnostics, consultation and treatment is indicated.
Non-apparatus-based examination
Also at the beginning of the examination in sleep medicine is the relevant collection of the patient’s medical history. This gives the sleep physician clues for possible diseases. Further clarity results from the evaluation of one or more special questionnaires to be filled out by the patients. In some cases a sleep diary is used, which has to be kept by the patient over a period of two weeks.
There is still a need for research regarding the collection of sleep-related medical history and the questionnaires used, in order to create generally accepted standards.
Apparatus-based investigations
A polysomnography is performed in a very similar way in children and adults.
Protocol of a polysomnography
Polysomnography is the basis of the instrumental examinations in the sleep laboratory, with the help of which sleep depth and sleep disorders can be determined. In the course of this examination, for example, the electrical activities of the brain (EEG) and heart (long-term ECG), the oxygen and carbon dioxide content of the blood, body temperature, respiratory flow and respiratory movement are continuously recorded, as well as muscle tension and leg and eye movements. In addition, it is not only possible to document special features such as erections, blood pressure, snoring sounds and gastric acid reflux, but also to make video recordings of the sleeper. In the case of sleep apnea syndrome, it is also possible to determine the appropriate ventilation pressure (breathing masks are used for therapy). Especially for the detection of this clinical picture, portable aids known as polygraph systems are available in addition to stationary facilities such as the sleep laboratory. Although these do not record electrical activity (brain waves), they do record parameters such as long-term ECG, oxygen content of the blood, movements during sleep and respiratory flow in the mouth and nose. However, these polygraph systems have almost 20% false negative and up to more than 30% false positive results and are therefore unsuitable for definitively confirming or rejecting the diagnosis of “sleep-related breathing disorders”. Here, too, there is a need for research.
Numerous different test procedures are available to determine a reduced performance due to the lack of restful sleep. There are clearly recommended procedures for their use. These include the d2 test, the Frankfurt Attention Inventory and the Oxford Sleep Resistance Test. Stationary driving simulators can also be used. Here, too, there is still a need for research.
Prevention
For prevention and treatment some facts are of fundamental importance. In industrialized countries sleep averages 7 hours, but can vary individually. Therefore every patient should find out for himself. Another important aspect is the correct behavior and handling of sleep, the so-called sleep hygiene. This also includes the correct and timely handling of the day-night rhythm.
Misconceptions about sleep
According to Volker Faust, these erroneous views are wrongly understood as norms:
“Eight hours sleep as a norm.” Correct: 6 to 7 hours or individually as needed.
“Older adults need more or less sleep than before.” Correct: Sleep becomes more susceptible to disturbances.
“Insomnia leads to mental illness.” Correct: Some mentally ill people can no longer sleep properly.
“Exertion before bedtime makes you tired.” Correct: Let the day end.
“Getting to sleep after a bad night’s sleep.” Wrong: Get up and work normally.
“Go to bed earlier if you have trouble falling asleep.” Wrong: Only go to bed when you are tired.
“If you wake up at night, stay in bed.” Wrong: Leave bed temporarily and relax.
“Those who cannot sleep should take sleeping pills.” Wrong: There is a danger of dependence.
“Full moon disturbs sleep.” Correct: Darken the light source.
Can one learn to get along with less sleep?
Normal eight-hour sleepers can maintain performance in the long term even with five to six hours of sleep. This requires a regular sleep-wake rhythm. For most people, this does not lead to long-term physical changes or damage. Such shortened sleep can improve quality. The person then sleeps more effectively, with complete preservation of deep sleep and shortened lighter sleep stages and REM sleep. The process of falling asleep is faster.
Treatment of Insomnia
Causal diseases must be treated by a healthcare professional. With sleep apnea syndrome, the use of positive pressure ventilation may also be necessary. Various substances such as drugs and medicines, but also stimulants such as alcoholic drinks, tobacco products or coffee can severely disturb the regulation of sleep and waking. For example, the epilepsy drug lamotrigine causes sleep disorders more frequently than other drugs such as pregabalin or levetiracetam for the same clinical picture. Here, a corresponding adjustment of lifestyle or the necessary medication is promising.
Sleep Substances
Sleeping pills approved for this purpose are primarily substances from the group of benzodiazepines, (non-benzodiazepine) hypnotics such as the Z drugs and chloral hydrate, opipramol, antihistamines as well as herbal medicines, which mostly contain valerian. Also, in some cases, antidepressants, where drowsiness is known as an additional effect, or weakly effective antipsychotics are used. The so-called interval therapy is recommended, especially to keep the side effects as low as possible and to prevent dependency: the patient may only take the medication on 2 or 3 days per week. Especially the continuous use of the drug has not yet been sufficiently investigated. In addition, in some cases these substances increase sleep disorders in the long term. Particularly with chronic sleep disturbances without recognizable organic cause therefore special value should be put on the weighing of use and risk. Other measures like the optimization of sleep hygiene for example by means of cognitive behavior therapy should be exhausted. For patients over 55 years with sleep disturbances without well-known cause melatonin, which seems to have certain therapeutic targets with disturbances of the sleep-awake rhythm, is available. The present study situation gives indications that also valerian has a certain sleep-promoting effect. There is no high-quality scientific proof and thus no evidence-based recommendation for the use of chloral hydrate, opipramol and antihistamines as sleep aids.
Behavioral therapy techniques
The following techniques can be used to treat sleep disorders:
Rules of sleep hygiene
Guide the structuring of the sleep-wake rhythm (stimulus control, sleep restriction).
Reduction of nocturnal musing through cognitive techniques.
Masturbation is also recommended to facilitate falling asleep.
Meditation: For primary insomnia, it may be worthwhile to try meditation. Deep relaxation techniques have been shown to prolong sleep time, improve sleep quality and make it easier to fall asleep (and stay asleep). These are some important facts about the practice that can help you overcome hesitation in trying it. Meditation can be a great tool for those who are looking for a natural, drug-free method to treat insomnia. In fact, meditation has been shown to help reduce the use of sleeping pills. The practice probably improves the insomnia symptoms by reducing the excitation measures in the brain. And there are no associated risks or side effects when you try meditation.

Meditation has been suggested to help with insomnia. Image copyright What the Fox Studio /IB Photography.
History of Insomnia Research
The beginnings of “quantitative” sleep research date back to 1862. At that time, Ernst Kohlschütter determined the depth of sleep and depicted it graphically in relation to sleep duration. For his experiment, he used acoustic stimuli of varying intensity and recorded the intensity at which his subjects woke up (wake-up threshold). Another milestone in basic research in this area is the electroencephalography (EEG) developed by Hans Berger. The use of electromyography and electrooculography made it possible to classify sleep into sleep stages as described by Allan Rechtschaffen and Anthony Kales in 1968.
The first classification system of sleep disorders appeared in 1979 under the title Diagnostic Classification of Sleep and Arousal Disorders. The classification was divided into four groups Insomnia (difficulties in falling asleep and staying asleep), hypersomnia (excessive sleepiness), disturbances of the sleep-wake rhythm and parasomnias (partial awakening and disturbances of sleep stages).
Urban Myths
Even in old medical publications, there are isolated statements that insomnia heralds an impending illness. Research has not been able to prove such a connection since then. A study published in 2015 by psychiatrist Aric Prather (UCSF) indicates that conversely, insufficient sleep promotes susceptibility to colds.